BY: JOANNA GRIGG
A top veterinarian sees Johne’s disease as the overlooked but potentially biggest curve ball to New Zealand’s agricultural image.
Johne’s disease is caused by the bacterium Mycobacterium avium subspecies paratuberculosis (MAP) and causes chronic enteritis in ruminant animals. The disease is responsible for significant economic losses worldwide. Vaccination can help improve the outcomes for animals and onfarm productivity.
Peter Anderson is an enthusiastic member of the Johne’s advisory group, a group of appointed scientists, veterinarians and agricultural industry representatives, charged with reviewing Johne’s science and raising issues with the wider industry.
The industry-funded Johne’s project (2016) showed 80% of NZ sheep flocks are infected, but only 18% of farms experience or are aware of any losses. Its undercover nature makes it easy for farmers to overlook it.
“I regard it as number one; it is potentially more of an issue than TB, as we are pretty well on top of that now.
“We need to be prepared to be able to show we are doing something and that Johne’s infections are declining.”
That something, he says, is vaccinating sheep. Vaccinating is one simple step to control the disease and bring profitability benefits to farms.
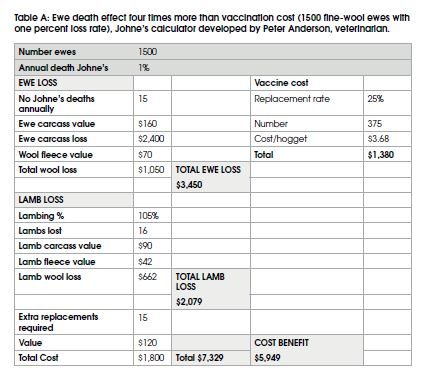
He calculates a one percent death rate in a flock of 1500 ewes costs $7300 to the flock each year (reduced sale of cull ewes and their wool, associated lamb loss, ewe replacement cost).
“This does not include the subclinical loss in wool and milk production and fertility from affected sheep that have not died.”
A vaccination for replacement hoggets would cost about $1300/year. This is a four-fold return on investment over the flock.
Anderson estimates 20% of fine wool flocks are vaccinated and a very low percentage of strong wool flocks. It used to require ear marking sheep but not now. However, farmers still need to notify meat processors if sheep have been vaccinated for Johne’s in their lifetime, on the animal status declaration (ASD) form.
 Care is required while vaccinating as self-injection can cause unpleasant reactions. Anderson suggests having a handler to help hold the animal still or using a conveyor with a crush are good ideas.
Care is required while vaccinating as self-injection can cause unpleasant reactions. Anderson suggests having a handler to help hold the animal still or using a conveyor with a crush are good ideas.
The number of vaccinations for Johne’s sold in NZ increased by 30% from 2018 and 2019, Anderson said, as farmers are starting to realise the production benefits.
“Farmers that start a vaccination programme soon start to appreciate the significant drop in missing sheep and the lack of scungy ewes that continually appear in the flock.”
The vaccination option, Gudair by Zoetis, is a single shot that can be given at any stage from tailing through to hogget selection. It costs about $3.68 per hogget. Vaccination will not eradicate the disease in a flock but seriously reduces shedding and the number that develop into cases and die.
“It’s a good option for flocks and we are crazy not to use it.”
Anderson said the world’s demand for healthy food means NZ may have a potential marketing advantage if they can be seen to be controlling Johne’s. The Johne’s advisory group keeps a watching brief on emerging research relevant to the sector both domestically and internationally. Recently, associations with Crohn’s disease in humans have been raised, however, further research is still needed by the international scientific community before any definitive conclusions can be drawn.
The Ministry for Primary Industries website document on ‘MAP & Crohn’s disease’ states evidence is inconclusive that MAP is a causative for Crohn’s disease and that the food safety control measures in place (pasteurisation of milk and good hygiene during slaughter) in NZ are appropriate. This hypothesis has been reviewed and investigated by the United Kingdom, Ireland and the European Union Food Safety Authorities.
While the issue simmers away in the background, Anderson said we need to be prepared to be able to show we are doing something and that Johne’s infections are declining.
Anderson also supports vaccination for dairy cows outside TB risk areas, with identity tags so they are then not tested for TB (they would be reactors due to the vaccination).
WHY VACCINATE REPLACEMENT HOGGETS FOR JOHNE’S?
• Improve health and welfare.
• Infected adult sheep shed bacteria onto pasture but may look fine (i.e. not scour).
• A vaccinated flock has reduced chance of developing the disease and shedding the bacteria. Young sheep are very susceptible.
• In a 2016 study, mortality from Johne’s averaged 2.8% in fine wool flocks and 0.4% for other breeds but there was a large property variation.
• By the time sheep die (three to four years) shedding has infected others.
• The one-shot-for-life vaccine costs about $3.68/head but rewarded with four-fold returns.
• Now a simpler process (no special ear mark required).
• May help solve the missing Merino wether issue.
JOHNE’S BEST PRACTICE
• Get tallies right to assess true loss.
• Vaccinate lambs at four weeks or at weaning, or at hogget selection. Earlier is best for high risk flocks.
• Blood test sheep (ELISA test) showing signs of wasting and cull immediately if ‘high positive’.
• Keeping the flock in good condition can minimise risk as stress from poor nutrition can trigger the disease.
• Don’t hang on to suspect Johne’s sheep – there is no cure and they are highly contagious.
• Don’t expose lambs to pastures grazed by wasting sheep or goats.
Missing sheep alarm bell
Fading ewes or wethers in the flock? Discrepancy between tallies, where you can’t find the carcases? Sheep fading despite feeding them better or drenching them?
These are all signs that Johne’s is impacting flock production.
To confirm, a post mortem is recommended. Johne’s shows as sheep in very poor condition with corded lymphatics, enlarged lymph nodes and thickened small intestine. This inflammation prevents absorption of nutrients and no cure is available.
Veterinarian Peter Anderson, said Johne’s can present with what was a fat twin-bearing ewe going downhill, losing her milk and lambs, and then succumbing herself.
“If you see one sheep dead there will be more.”
He recommends starting a vaccination programme, with the ideal time to inject being post-shearing or hogget selection.
“Vaccination doesn’t prevent infection but does prevent disease.”
“It reduces the clinical cases of the disease,” he said.
A sheep mortality study (2016) funded through the Johne’s research consortium (industry and government funds) showed that the vaccine efficacy was 72%. This was across 20 flocks in both the North and South Islands over two years. In all these flocks, some of which were vaccinating or had partially vaccinated the flock, none of the sheep with clinical Johne’s were vaccinated animals.
The benefit of vaccinating ewe lambs in a fine wool flock was calculated at 5.4 times the cost. It also paid for other stronger wool breed flocks, even though the mortality rate prior to treatment was only 0.7% of the flock. The benefit was still 1.6 times the cost. This was only the loss from ewe deaths and did not include the subclinical losses from reduced ewe performance.
Merino and Merino cross breeds were more susceptible and suffered a greater production loss than other breeds.
A much earlier study (1980s) of Romney, Merino and Merino-cross genotypes studied 3500 ewes over eight years. In their final year of production, ewes with clinical Johne’s disease had 5.3kg lower liveweight, half a kilo less wool and 13% fewer lambs born and lower litter weaning weights, compared with clinically normal ewes. Over the eight years of monitoring, 3.5% of Romney ewes and 4.8% Merino and Merino-Romney cross ewes were diagnosed with clinical Johne’s disease. Annually this is 0.9% and 1.2% of the mobs. Clinical Johne’s disease led to significant losses in bodyweight, greasy fleece weight and number of lambs born in the lifetime production of ewes. Overall, there was a 46% reduction in productivity.
Loss of production coupled with animal welfare, combine to make a strong
case for vaccination, whatever the sheep breed.
FARMERS RESTART VACCINE
Tim and Sally Wadworth, say their Merino flock will continue to be vaccinated for Johne’s as the benefits are so obvious; both visually and financially.
The Marlborough hill country farm Aschworth started a vaccination programme for ewe lambs in 1994. At that time, it was a live vaccine that had to be mixed and administered very carefully. Each lamb was tipped up and the vaccine injected into the cheek muscle. It received a special earmark for identification, which was then a legal requirement.
Five years on, Johne’s had visually disappeared from the flock.
“We were now in a situation where we were losing very few sheep and production had increased,” said Tim.
After vaccinating for about 15 years and with very little stock loss, an increase in production and wool weight, and with no apparent sign of Johne’s, they decided to stop vaccinating. But slowly Johne’s returned.
Over four to five seasons, the Wadworths noticed a higher incidence of individual sheep in poor condition. The vaccination programme was rebooted.
Vaccination is slightly easier now, Tim said, with a different product and method of injection but still requiring extreme care.
“Like all vaccines they will only work if administered correctly.”
Vaccinations are given to replacement hoggets at shearing, straight off the shears, in the shed. The experience has left the Wadworths committed to annual vaccination of all young capital stock.



